From the start of quarantine, media sources from the Wall Street Journal to the New York Times made a basic assumption that all reopening policy must be expedited because our collective mental health was at risk. Many pieces proclaimed a “mental health tsunami” and “mental health pandemic” was in our future unless we took serious steps to return everyone back to their starting places. Of course, this seemed like a reasonable assumption to make.
We have all been under stress, while feeling lonely and grieving. Many people have lost employment, income and loved ones. It would seem logical that widespread mental health problems would soon arrive if we couldn’t make a quick return to “normal.”
Still, I found myself curious. I have studied the effects of trauma and stress on individuals, families and communities for nearly two decades. I have investigated the impacts on children and their families after they experience the stress and trauma associated with living in poverty, sudden grief and loss, family violence, disaster.
What I know to be true is this: 1) people, and especially children, can be incredibly resilient; 2) healthy relationships matter most to what makes people, and especially children, resilient; and 3) the negative effects of trauma are rarely a function of a single risk factor or event, but rather the total sum of additional stressors that surround the risk factor or event and the presence of resources to cope and maintain resilience.
Thus, could this single risk factor, lockdown — cataclysmic as it was — be the single predictor of a mental health tsunami?
A group of researchers has answered this question: no.
In a recent meta-analysis of 2,158 studies on a multitude of mental health outcomes, including depression, anxiety, posttraumatic stress disorder, sleep disturbances, substance use, and suicidality, completed globally between January 2020 and June 2020, the effects of lockdown are quite small in their impact on mental health.
There was a small but significant uptick in depression and anxiety and even smaller, non-significant effects of lockdown on suicide risk. There were also very small, negative but non-significant impacts on positive functioning, including people’s perceptions of their social support. Besides the mental health effects being small, the researchers pointed out they were quite heterogeneous.
In other words, changes in mental health at the population level are more likely related to person-centered factors, like preexisting mental health problems, illness, and economic adversity, than an implication of general and widespread experiences like quarantine. The researchers explain their non-significant findings as a function of this heterogeneity as well as a function of the great human capacity for resilience. It’s also true that the pandemic and related quarantine are not the only social factors to predict mental health functioning.
We have endured many struggles over the last year, and the latest research helps form a more complex story of the mental health problems we currently face, have faced, and where we go from here.
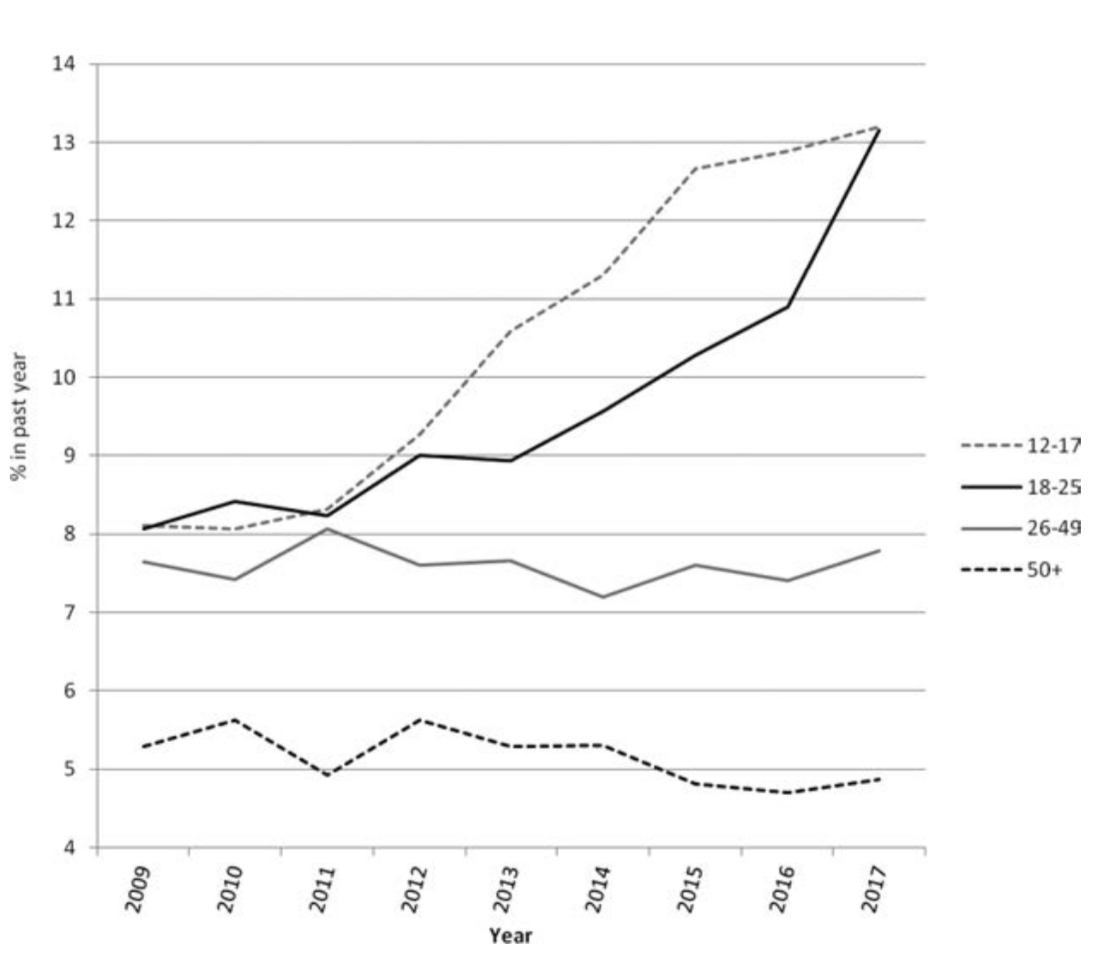
Mental health problems have long been a public health problem that has only escalated over time, a trend independent of the current pandemic. In 2019, 1 in 5 U.S. adults and 1 in 6 U.S. children suffered from a mental health problem. Suicide was the second leading cause of death for adolescents. Younger people may be at particular risk for psychological distress. Rates of a major depressive episode experienced in a given year increased 52% between 2005 and 2017 among teens 12-17 years old.
To put it all in context, the effects of exposure to stressors associated with poverty, domestic violence, and parental mental health problems are all known to make larger impacts on children’s mental health. There is some evidence that there was an uptick in each of these areas of risk over the last year, but it’s a challenge to fully contextualize these changes.
Reported spikes in family violence, for example, are of great concern, but reports may fail to fully capture seasonal effects as well as long-term trends. There has been a steady increase in domestic violence reports since 2014, after many years of steady declines in violence after the Violence Against Women Act (VAWA) was passed. VAWA has failed reauthorization in recent years, including during 2020 when public concern about domestic violence seemed to expand.

Racism makes a larger overall impact on mental health, too. Science is catching up with what has long been known by Black individuals and communities in particular, as well as by other individuals and groups impacted by the harm of White supremacy, and the period of quarantine has brought rise to a national reckoning. On numbers alone, might we see the same widespread hand wringing about racial justice that we have on quarantine? I would hope so if, in fact, what we are most concerned about is the mental health crisis.
We got it wrong. We got it wrong — and we’d be wise to reconsider our policy response, still ongoing at multiple levels.
That is, assuming the broad concern over mental health is authentic and not just a useful talking point. We were a country with serious mental health problems and only modestly effective intervention strategies before March 2020. The intervention issue speaks to the complicated nature of mental health disorders. The risk factors for the development of mental health problems interact across biopsychosocial levels and are rarely pinned to a single indicator.
Reopening and removing public health restrictions may buffer some of the difficult feelings many of us have had over the last year, but to truly impact the ongoing mental health crisis — to the extent that’s the goal — much more is needed at the systems level.
Improving access to mental health care, meaningfully addressing racial and economic justice, shifting away from police as first responders, and investing in children from birth are data-driven strategies to make mental health the national priority it would already have been in a just world.
Comments
Sign in or become a Nu?Detroit member to join the conversation.
Just enter your email below to get a log in link.